 Medical Billing
Medical Billing Medical Coding
Medical Coding Medical Audit
Medical Audit Provider Credentialing
Provider Credentialing Denial Management
Denial Management A/R Follow-up
A/R Follow-up Private Practice
Private Practice Patient Help Desk
Patient Help Desk Customized Reporting
Customized Reporting Out-of-Network Billing
Out-of-Network Billing Internal Medicine
Internal Medicine Pediatrics
Pediatrics Radiology
Radiology Surgery
Surgery Emergency Medicine
Emergency Medicine Anesthesiology
Anesthesiology Cardiology
Cardiology Orthopedic
Orthopedic Psychiatry
Psychiatry Dentistry
Dentistry OB-GYN
OB-GYN Family Medicine
Family Medicine
Remote Patient Monitoring (RPM) is transforming chronic care with real-time patient tracking, improving outcomes, care continuity, and managing conditions like diabetes, hypertension, and cardiac diseases. Driven by Medicare expansion, RPM adoption has grown by 40%+ in the past three years, with a 15–25% reduction in hospital readmissions.
However, billing has not kept pace. Around 20–30% of RPM claims are delayed or denied due to documentation, time-tracking, and coding errors, leading to revenue leakage and payment delays. As RPM scales in 2026, accurate billing and compliant revenue cycle management are essential to protect revenue. Read the full blog to avoid RPM billing challenges and secure reimbursements.
Why RPM Billing Is More Complex Than Traditional Medical Billing
Remote Patient Monitoring (RPM) is transforming care delivery, but when it comes to billing, it introduces a level of complexity that traditional medical services simply don’t have. Unlike standard fee-for-service visits that are billed once per encounter, RPM revolves around continuous patient monitoring, where reimbursement depends on ongoing data collection, device usage, and time-based clinical engagement throughout the month.
This is where most practices begin to struggle. CMS requires at least 16 days of recorded patient data within a 30-day billing cycle for RPM reimbursement eligibility. On top of that, certain RPM CPT codes demand a minimum of 20 minutes of clinical interaction time per month. These may seem like small thresholds, but even minor gaps in tracking or documentation can lead to automatic claim denials or reduced payments, turning otherwise successful patient monitoring into lost revenue.
The challenge doesn’t end there. RPM billing becomes even more complicated due to inconsistent payer rules across the healthcare landscape. Studies show that more than 60% of providers experience confusion around differing RPM billing requirements, resulting in coding inconsistencies, delayed reimbursements, and higher denial rates. In practice, this means that even when care is delivered correctly, revenue is often not captured correctly, making RPM billing one of the most operationally sensitive areas in healthcare revenue cycle management today.
RPM Billing Workflow: Step-by-Step Process for Clean Claims
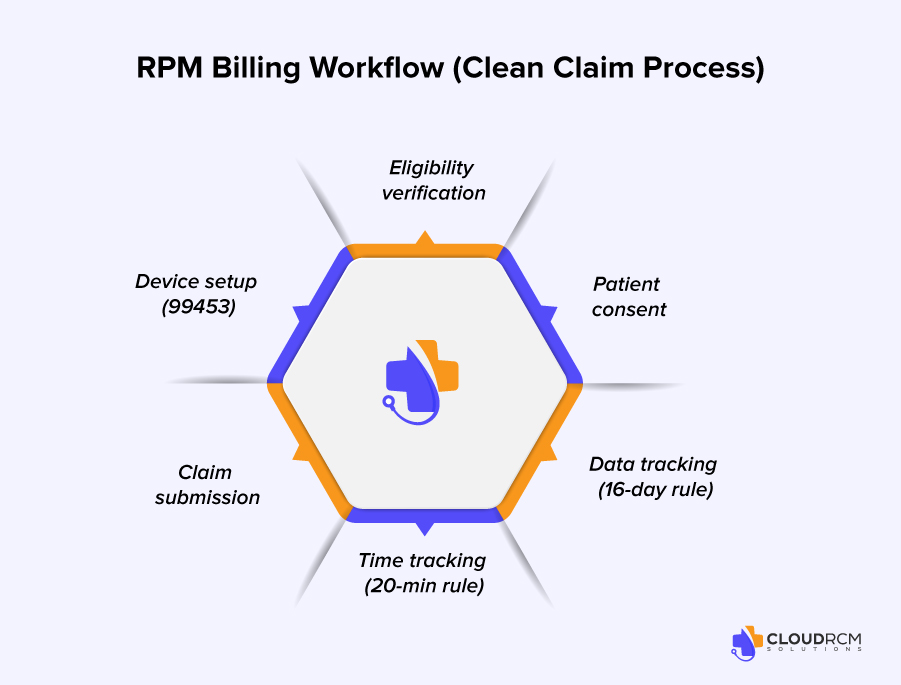
A well-defined RPM billing workflow is essential for reducing errors, improving compliance, and ensuring consistent reimbursement. In 2026, successful RPM programs are built on structured, repeatable processes that connect patient care with accurate billing execution.
The process begins with patient eligibility verification, ensuring that the patient qualifies under CMS RPM guidelines. This is followed by documented patient consent, which is mandatory before initiating any RPM billing activity.
Once enrolled, providers must complete device setup and patient education in alignment with CPT 99453. As monitoring begins, practices must track device-generated data to meet the 16-day requirement under CPT 99454 while simultaneously documenting clinical interaction time to satisfy CPT 99457 requirements.
Finally, all documentation and time logs must be validated before claim submission. Any breakdown in this workflow can result in RPM claim denials, delayed payments, or revenue leakage.
Practices that implement structured workflows experience fewer billing errors, faster reimbursements, and improved RPM revenue cycle performance.
Key RPM CPT Codes Providers Must Understand
RPM billing success starts with one critical factor: understanding how each CPT code drives reimbursement. In 2026, Remote Patient Monitoring is no longer just about collecting data; it’s about proving compliance, documenting engagement, and accurately capturing every billable element of the care process. When these codes are misunderstood or inconsistently applied, even well-run RPM programs can quickly turn into revenue leakage.
Each CPT code represents a specific stage of the RPM journey, and payers expect clear, time-stamped, and well-documented evidence for every step from onboarding to ongoing clinical interaction. As RPM programs scale, even small documentation gaps or timing errors can trigger denials, delays, or underpayments.
Below is a simplified breakdown of the most critical RPM CPT codes providers must master:
| CPT Code | Description | Key Billing Requirement | Common Billing Risk |
| 99453 | Device setup and patient onboarding | One-time setup with documented patient education and device initiation | Missing onboarding proof or incomplete setup documentation |
| 99454 | Device supply and data collection | Minimum 16 days of physiologic data within a 30-day billing cycle | Insufficient data transmission or device inactivity |
| 99457 | Clinical management and interactive communication | At least 20 minutes of patient interaction per month | Underdocumented time or missing communication logs |
| 99458 | Additional clinical management time | Incremental billing for each additional 20-minute segment | Incorrect time aggregation or unsupported billing entries |
RPM vs CCM vs RTM Billing: Understanding the Key Differences
As remote care services continue to expand in 2026, many providers struggle to differentiate between Remote Patient Monitoring (RPM), Chronic Care Management (CCM), and Remote Therapeutic Monitoring (RTM). While all three programs support patient care outside traditional visits, their billing structures, documentation requirements, and reimbursement models are significantly different.
RPM billing focuses on the collection and analysis of physiological data such as blood pressure, glucose levels, and heart rate using connected medical devices. Reimbursement is tied to device data collection, patient engagement, and time-based clinical interaction under CPT codes like 99453, 99454, and 99457.
In contrast, CCM billing is centered around care coordination for patients with multiple chronic conditions, without requiring device-generated data. It relies heavily on care plan management, medication coordination, and monthly non-face-to-face services, typically billed under CPT 99490.
RTM billing, on the other hand, is designed for therapy-based monitoring, including musculoskeletal and respiratory conditions. Unlike RPM, RTM allows the use of patient-reported data and is often utilized by physical therapists and non-physician providers.
Understanding these differences is critical because incorrect program selection or improper CPT usage can lead to RPM claim denials, compliance risks, and lost reimbursement opportunities.
Common RPM Billing Challenges Leading to Claim Denials
Remote Patient Monitoring (RPM billing 2026) continues to unlock strong revenue opportunities, but RPM claim denials remain a major barrier for providers. Despite increased adoption, many practices still struggle with RPM reimbursement due to documentation gaps, time tracking issues, and payer-specific billing rules under strict CMS RPM guidelines. Even small workflow errors can result in lost revenue, delayed payments, or complete claim rejection.
1. Documentation Gaps and Missing Clinical Records
Incomplete RPM documentation causing billing breakdowns
One of the most common reasons for RPM claim denials is missing or incomplete clinical documentation. Providers are required to consistently capture patient consent, device-generated data, and clinical interaction notes to support RPM CPT codes. When even one element is missing, claims often fail payer validation.
Why does it lead to RPM revenue loss?
Poor documentation is responsible for nearly 35% of RPM billing denials, making it one of the biggest threats to RPM reimbursement. In most cases, the clinical work is completed, but revenue is lost due to documentation failures in RPM revenue cycle management.
2. Time-Based Billing Compliance Issues (20-Minute Rule)
RPM CPT 99457 billing time requirements
RPM reimbursement under CPT 99457 requires at least 20 minutes of interactive communication per patient per month. However, many practices struggle with accurately capturing this time due to manual workflows or inconsistent logging.
Impact on reimbursement accuracy
Failure to meet or document the 20-minute threshold leads to underbilling or outright RPM claim denials. This makes time tracking one of the most critical compliance factors in RPM billing systems today.
3. Patient Enrollment and Consent Errors
Missing RPM consent and onboarding documentation
Every RPM program begins with proper patient enrollment, but missing consent forms or incomplete onboarding records are still common issues. These errors directly affect eligibility under RPM CPT 99453 requirements.
Direct impact on claim approval
Without valid consent documentation, RPM claims can be immediately denied. Industry data shows that 15–20% of RPM revenue loss is linked to enrollment and consent failures, making this a high-risk billing gap.
4. Failure to Meet Device Data Requirements (16-Day Rule)
CMS RPM 16-day data compliance requirement
Under CMS RPM guidelines, providers must collect at least 16 days of device-generated data within a 30-day billing cycle to qualify for reimbursement under CPT 99454.
How data gaps lead to RPM claim denials
Device inactivity, poor connectivity, or patient non-adherence can result in insufficient data collection. Even minor gaps can make the entire RPM billing cycle non-reimbursable, leading to direct revenue loss.
5. Payer Variability and Confusing Billing Rules
Inconsistent RPM reimbursement policies
RPM billing is not standardized across all payers. Medicare, Medicaid, and commercial insurers often have different interpretations of RPM CPT codes, documentation rules, and approval criteria.
Effect on RPM revenue cycle management
This inconsistency leads to coding errors, delayed payments, and increased RPM claim denials. For multi-payer practices, managing RPM reimbursement becomes significantly more complex without standardized workflows.
6. Incomplete Patient Engagement Tracking
Breakdowns in RPM monitoring visibility
Even when RPM devices are correctly deployed, many practices fail to maintain continuous visibility into patient engagement. Without consistent tracking, it becomes difficult to confirm eligibility for billing.
Risk to RPM billing accuracy
Since RPM reimbursement depends on ongoing patient participation, incomplete engagement tracking increases claim rejection risk and creates compliance vulnerabilities.
7. Fragmented Documentation Across Multiple Systems
Disconnected RPM billing and clinical systems
Many healthcare organizations still use separate platforms for EHRs, RPM device data, and billing workflows. This creates fragmented documentation and increases the risk of missing or duplicate records.
Delays in RPM reimbursement processing
Billing teams often spend hours reconciling data across systems, which slows down claims submission and leads to delays in RPM revenue cycle management.
8. Delayed Clinical Communication Logging
Missed real-time RPM interaction documentation
Interactive communication between providers and patients must be properly documented for RPM CPT 99457 billing. However, in busy practices, these interactions are often logged late or inconsistently.
Underreported clinical time and lost revenue
When communication is not documented in real time, billable RPM time is lost, directly reducing monthly RPM reimbursement.
9. Device Connectivity and Data Transmission Gaps
Unstable RPM device performance
Patients may experience poor connectivity, device errors, or inconsistent usage, especially in elderly or high-risk populations.
Failure to meet CMS data thresholds
Even a few missing days of data can result in failure to meet the 16-day requirement, making the entire RPM billing cycle non-billable under CMS RPM guidelines.
10. Staff Overload and Manual RPM Workflows
High administrative burden in RPM billing operations
RPM programs significantly increase workload for clinical and billing staff, including eligibility verification, documentation, time tracking, and claim preparation.
Increased errors and slower reimbursements
Manual processes increase human error, delay claim submissions, and contribute to higher accounts receivable (AR) days, negatively impacting RPM revenue cycle performance.
Why These RPM Billing Challenges Matter in 2026
RPM billing challenges are no longer just administrative issues; they directly affect revenue integrity, compliance risk, and practice profitability. As CMS RPM guidelines tighten and payer audits increase, healthcare organizations that fail to optimize RPM billing workflows face higher denial rates and reduced reimbursement.
In contrast, practices that adopt automated RPM billing systems, standardized documentation processes, and integrated patient engagement tools are better positioned to achieve consistent RPM reimbursement and long-term financial stability.
RPM Billing Audit Checklist for Clean Claims and Compliance
Before submitting any RPM claim, providers must ensure that all compliance and documentation requirements are fully met. Even minor gaps can result in claim denials or audit exposure.
- Patient eligibility verified under current CMS RPM guidelines
- Documented patient consent linked to RPM enrollment
- Device setup and education completed under CPT 99453
- Minimum 16 days of device data recorded under CPT 99454
- At least 20 minutes of documented interaction for CPT 99457
- Accurate time tracking and logs for additional CPT 99458 usage
- Payer-specific billing requirements reviewed before submission
Practices that use a structured RPM billing checklist significantly improve claim accuracy, reduce denial rates, and maintain compliance with evolving RPM billing regulations.
Common RPM Denial Codes and What They Really Mean
Understanding why claims are denied is just as important as knowing that they are denied. In remote patient monitoring billing, denial patterns often follow predictable coding and documentation gaps. Mapping these denials to root causes allows providers to fix issues at the workflow level not just resubmit claims.
| Denial Code | Meaning | Root Cause in RPM Billing | Prevention Strategy |
| CO-16 | Missing or incomplete information | Missing consent, incomplete documentation, or lack of interaction logs | Standardize RPM documentation and ensure all required fields are captured before submission |
| CO-50 | Medical necessity not proven | Lack of documented clinical need for RPM services | Strengthen medical necessity documentation and link RPM to chronic condition management |
| CO-97 | Service not covered / bundled | Incorrect code usage or payer-specific exclusions | Verify payer-specific RPM billing guidelines before claim submission |
| CO-29 | Timely filing issue | Delayed claim submission due to workflow inefficiencies | Implement faster claim submission cycles and automated tracking |
| CO-197 | Precertification/authorization issue | Missing prior authorization (for certain payers) | Verify eligibility and authorization requirements before enrollment |
Best Practices to Reduce RPM Billing Errors and Improve RPM Reimbursement in 2026

To succeed in remote patient monitoring billing in 2026, providers must shift from reactive corrections to proactive RPM revenue cycle management built on automation, accuracy, and compliance.
- Standardize RPM documentation workflows to ensure every claim meets CMS audit requirements and passes payer validation on first submission
- Automate time tracking to capture every billable minute under CPT 99457 and prevent hidden revenue loss
- Monitor the 16-day threshold in real time to eliminate non-billable cycles before they impact reimbursement
- Strengthen onboarding workflows to reduce 15–20% revenue loss linked to consent and enrollment errors
- Track payer-specific rules to prevent avoidable denials across multi-payer environments
When these strategies are implemented together, practices see lower denial rates, faster reimbursements, and stronger RPM revenue performance.
RPM Revenue Potential: How Much Can Your Practice Earn?
Remote Patient Monitoring is not just a clinical tool; it is a recurring revenue opportunity when billing processes are optimized. However, the financial success of RPM programs depends on accurate documentation, compliance, and consistent patient engagement.
On average, practices generate between $120–$180 per patient per month through RPM services, depending on utilization and CPT code usage. For example, managing 100 active RPM patients can generate approximately $12,000 to $18,000 in monthly revenue.
However, this potential is often reduced by RPM billing errors such as missing documentation, failure to meet the 16-day data requirement, or incomplete time tracking. Even a small percentage of denied claims can significantly impact profitability.
Practices that optimize RPM billing workflows through automation, standardized documentation, and proactive denial management achieve more predictable revenue, faster reimbursements, and stronger financial performance.
Emerging RPM Billing Trends in 2026
The future of RPM billing is being shaped by automation, artificial intelligence, and stricter compliance frameworks. Providers who adapt early will have a significant financial and operational advantage.
1. AI-Driven RPM Revenue Cycle Management
Artificial intelligence is transforming RPM billing by automating documentation review, identifying missing data, and flagging potential RPM claim denials before submission. This reduces administrative workload while improving billing accuracy.
2. Expansion of CMS RPM Guidelines and Compliance Requirements
CMS continues to refine RPM billing regulations, placing greater emphasis on real-time data accuracy, patient engagement tracking, and interoperability across EHR systems. These updates are expected to further tighten RPM reimbursement standards in 2026 and beyond.
3. Growth of Hybrid Care and Remote Monitoring Models
Healthcare is shifting toward hybrid care models that combine in-person visits with continuous RPM monitoring. This shift is increasing RPM adoption across cardiology, endocrinology, and primary care, making RPM billing a core revenue stream rather than a secondary service.
4. Integration of RPM with Patient Engagement Systems
Modern RPM programs are increasingly integrated with patient engagement platforms to improve adherence, reduce data gaps, and ensure consistent device usage. This integration directly improves RPM reimbursement outcomes and reduces claim denial rates.
Why CloudRCM Solutions Is the Right Partner for RPM Billing Success
CloudRCM Solutions transforms complex RPM billing into a streamlined, revenue-generating system by aligning patient engagement, clinical documentation, and reimbursement workflows into one unified strategy. Instead of dealing with recurring RPM claim denials, missed billing opportunities, and compliance risks, providers gain a fully optimized RPM revenue cycle designed for accuracy, speed, and scalability. With end-to-end RPM billing support, automated documentation and time tracking for CPT 99453, 99454, 99457, and 99458, proactive denial prevention, and faster reimbursement cycles, practices can eliminate revenue leakage and maximize monthly recurring RPM revenue. In an environment where CMS regulations and payer scrutiny continue to tighten, CloudRCM Solutions ensures your RPM program remains compliant, efficient, and consistently profitable.
Conclusion
RPM billing in 2026 is no longer just a documentation task; it’s a direct driver of revenue performance. Practices that continue relying on manual workflows, inconsistent documentation, and reactive billing processes will keep losing 20–30% of their potential RPM revenue to preventable denials and inefficiencies.
On the other hand, providers who invest in structured, automated, and compliance-driven RPM revenue cycle management are building predictable, scalable revenue streams with faster reimbursements and lower operational risk. CloudRCM Solutions helps you close these gaps by turning complex RPM billing into a streamlined, high-performance system built for accuracy, compliance, and growth.
If your practice is experiencing RPM claim denials, delayed payments, or revenue leakage, now is the time to fix the foundation. Partner with CloudRCM Solutions to reduce denials, accelerate reimbursement, and unlock the full revenue potential of your RPM program in 2026 and beyond.
What are the most common RPM billing challenges?
The most common challenges include documentation errors, failure to meet time-based CPT requirements, patient consent issues, and payer policy variability.
Why are RPM claims denied?
RPM claims are often denied due to missing documentation, incorrect CPT codes, insufficient monitoring time, or failure to meet payer-specific requirements.
How much revenue can RPM generate per patient?
RPM programs typically generate between $120–$180 per patient per month, depending on service utilization and billing accuracy.
How can providers reduce RPM billing errors?
Providers can reduce errors by using automated tracking systems, standardizing workflows, and ensuring compliance with billing guidelines.
What documentation is required for RPM billing compliance?
RPM billing requires documented patient consent, device setup details, at least 16 days of device data, and a minimum of 20 minutes of clinical interaction per month to meet CMS RPM guidelines.
What happens if the 16-day RPM requirement is not met?
If the required 16 days of device data are not recorded within a 30-day period, providers cannot bill CPT 99454, making the entire billing cycle non-reimbursable.
Can RPM and CCM be billed together?
Yes, RPM and Chronic Care Management (CCM) can be billed together if all CMS requirements for both services are met and proper documentation supports each service independently.


